Bone building in Munich
When is a bone structure (= augmentation) necessary?
Bone building is useful wherever bone loss has occurred. Especially where new functional dentures with implants are planned, sufficient bone volume plays an important role.
Bone structure can also be useful in exceptional situations, where only a bridge replacement is planned by an atrophy (= bone loss) but must be expected with an ugly degradation.
A bony jaw structure can be done in many ways. This is determined on the one hand by the extent of bone loss and the planned form of replacement. Based on many years of experience in science and research, we offer numerous possibilities for restoring lost bone in our practice. The effort and the right choice of the method depends largely on the initial situation.
Therefore, it makes sense to explain the various measures to the patient on the basis of the defect size present. Accurate diagnostics (from X-rays to clinical examination to 3D analysis) will tell you exactly what form and extent bone loss is and how it can be repaired.
In a detailed consultation with your dentist in Munich, we will explain the possible measures exactly. Based on this conversation, you will receive a detailed and accurate schedule and cost plan.
Ridge atrophy – bone loss after tooth loss.
What does that mean and how can you prevent it??
After a tooth loss you can observe a decrease of the bony ridge after a relatively short time. This process is reinforced by wearing a removable mucosal denture (partial denture, full denture). In order to reduce this for the transition from the healing phase after tooth removal to implantation, we provide our patients with the innovative technique of an elastic thermoplastic prosthesis (Valplast). This is comfortable to wear and reduces pressure on the jaw and adjacent teeth (if any).
The principle of atrophy is clearly understandable. Human bone is subject to dynamic processes. Where it is needed, it is reinforced – where the load is missing and possibly even added a pressure load, it is degraded – similar to the muscle tissue.
Therefore, dental implants are an important factor in generating again tensile forces in the bone that reinforce the bone around the implants. Therefore, after a tooth loss, it should not be too long to wait to decide on the implant placement. This can be useful right after pulling for up to 4 months after removing a tooth. It may also be useful to secure the tooth cavity from tooth atrophy by means of a special membrane and / or bone substitutes (socket preservation).
Depending on the initial situation, we will give you the ideal implantation time from a medical-biological and dental point of view.
More information about bone structure:
Why a bone implantation is often required in a dental implantation.
 To ensure that an implant can be anchored securely for as long as possible, the presence of a sufficient volume of jawbone plays a crucial role. If this bone is no longer in sufficient width or height, it must be restored to achieve a durable stable result.
To ensure that an implant can be anchored securely for as long as possible, the presence of a sufficient volume of jawbone plays a crucial role. If this bone is no longer in sufficient width or height, it must be restored to achieve a durable stable result.
If dental implants are placed in too small a bone volume, complications can often occur only after years. Similar to a dowel, which loosens only after years of stress, if this was not set sufficiently dimensioned. The consequences of loose dental implants are usually severe and can only be treated with great effort.
If the volume of the jawbone is not clear, we use a three-dimensional image. With our modern DVT device, we can perform such a recording with low radiation and concentrated on only one jaw section.
Thus, we increase the safety in diagnostics and planning, and can explain to you in advance of the treatment, the scope and the alternatives exactly.
Bone building – how does the oral surgeon / implantologist do that?
 From our practice and according to the findings of current studies, it is necessary for the placement of sufficiently sized dental implants (the size of the dental implants should be based on the size of the lost teeth!) In about 50% of cases, to build up a bone before or during implantation.
From our practice and according to the findings of current studies, it is necessary for the placement of sufficiently sized dental implants (the size of the dental implants should be based on the size of the lost teeth!) In about 50% of cases, to build up a bone before or during implantation.
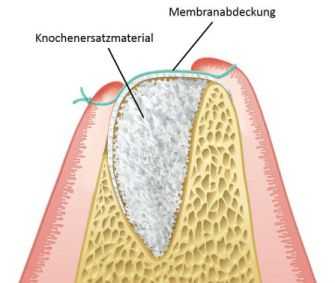
If the alveolar ridge dimension is still adequate, the implant can be used immediately if the bone loss is low to moderate (due to atrophy or inflammation). With intrinsic bone chips (which are atraumatically obtained during the procedure) and / or a bone substitute material, the missing bone can be built around the implant. To secure the structure, a protective membrane is placed over the structure in many cases. This membrane is usually absorbable, that is, it dissolves in the healing phase and supports the formation of a new periosteum. If necessary, this cover is additionally fixed with tiny nails (pins).
This technique (membrane technique) is also used in many other, more elaborate methods of bone formation.
If you are interested in the different methods used, we would like to explain them in the following overview:
The different procedures of bone reconstruction – explained by your specialist for oral surgery and implantology in Munich:
- Use of bone substitute material and membranes
- Bone Splitting / Bone Splitting
- Bone condensation / Bone Condensing
- Sinus lift, Sinusbodenaugmentation = bone structure of the antrum
- Socket Preservation
- Bone block augmentation (self-bone grafting / donor block / CAD block)
Use of bone substitute material and membrane
 For smaller defects or low atrophy, the jaw can be reconstructed in its shape by placing its own bone at the surgical site mixed with bone replacement material around the implant and into the defect. For larger defects or a defective periosteum, this structure can be covered with a membrane. So the regeneration can proceed undisturbed. The membranes are broken down without residue by the body. Necessary fasteners (pins) can be removed later.
For smaller defects or low atrophy, the jaw can be reconstructed in its shape by placing its own bone at the surgical site mixed with bone replacement material around the implant and into the defect. For larger defects or a defective periosteum, this structure can be covered with a membrane. So the regeneration can proceed undisturbed. The membranes are broken down without residue by the body. Necessary fasteners (pins) can be removed later.
However, bone substitute material may also be used in far larger defects or in bone augmentation processes of the antrum (e.g., sinus lift).
Bone Splitting / Bone Splitting
 If the jawbone is too narrow and an implant can not therefore be introduced primarily into the bone without a larger exposure (exposure), the bone splitting may represent a suitable solution to the problem. With the help of fine saws and chisels, the jaw bone is separated (separated) and the two lamellae are stretched apart. Between the two slats then a gap is formed in which the dental implant is introduced. The remaining cavities are then filled with autologous bone and bone substitute material. Thereafter, a membrane cover as described above. In our practice clinic, we no longer use saws to separate the narrow alveolar ridge, but use the innovative piezoelectric technology known in bone surgery. With micro-vibrations, the bone is cut without disturbing vibrations and without harmful heat development. A procedure that we have been successfully using for years in oral surgery.
If the jawbone is too narrow and an implant can not therefore be introduced primarily into the bone without a larger exposure (exposure), the bone splitting may represent a suitable solution to the problem. With the help of fine saws and chisels, the jaw bone is separated (separated) and the two lamellae are stretched apart. Between the two slats then a gap is formed in which the dental implant is introduced. The remaining cavities are then filled with autologous bone and bone substitute material. Thereafter, a membrane cover as described above. In our practice clinic, we no longer use saws to separate the narrow alveolar ridge, but use the innovative piezoelectric technology known in bone surgery. With micro-vibrations, the bone is cut without disturbing vibrations and without harmful heat development. A procedure that we have been successfully using for years in oral surgery.
Bone condensation / Bone Condensing
This method describes a special way of preparing the implant bed. Especially in the upper jawbone one often finds a very wide-meshed and thus also “yielding” bony structure. The basis of successful implant healing is the primary strength of the dental implant after it has been implanted. If the bone is very soft, this primary stability may not be sufficient. Bone Condensing does not remove the bone with drills, but compresses it using special instruments. Since Dr. Schmidt (implantologist since 1999) has been working on this method for improving the success prognosis of implants for a long time, he has developed his own instruments for this procedure.
For more information about this generally unknown method, see WIKIPEDIA. Here is Dr. Achim Schmidt wrote a corresponding article on bone compaction.
Socket Preservation
 This relatively new technique describes the process of preserving the bony structures immediately after a tooth extraction. This technique is used when after a tooth removal due to the thin tooth walls with a relatively rapid absorption (bone degradation) must be expected. In order to keep the volume of the bone stable, the tooth socket (alveolus) is filled with a bone substitute material immediately after removal of the tooth and covered with a membrane.
This relatively new technique describes the process of preserving the bony structures immediately after a tooth extraction. This technique is used when after a tooth removal due to the thin tooth walls with a relatively rapid absorption (bone degradation) must be expected. In order to keep the volume of the bone stable, the tooth socket (alveolus) is filled with a bone substitute material immediately after removal of the tooth and covered with a membrane.
Here we often use a foil which, unlike the membrane techniques described above, is not resolving. This special membrane of high-density Teflon (PTFE) is bacteria-proof and can be removed like a plaster after a short time of about two to three weeks. The underlying tissue is already stable. In this way, unwanted, rapidly ingrowing granulation tissue (= repair tissue) is blocked already in the initial phase. The complete ossification of the tooth compartment can be done unhindered and quickly.
Bone block augmentation
(Self-bone grafting / donor block / CAD block)
If there is a large bone deficit after a major inflammatory process, trauma or very advanced atrophy, this can not be reliably reconstructed with the measures described above.
 In such cases, the affected jawbone section can only be built up with a bone block. This is adapted to the site and fixed with special screws. After fixation, the transitions with bone augmentation material are compensated and a cover with a resorbable membrane. After a healing period of three to five months, the fastening screws are removed and the dental implants can be inserted into the newly formed bone.
In such cases, the affected jawbone section can only be built up with a bone block. This is adapted to the site and fixed with special screws. After fixation, the transitions with bone augmentation material are compensated and a cover with a resorbable membrane. After a healing period of three to five months, the fastening screws are removed and the dental implants can be inserted into the newly formed bone.
This procedure is extremely difficult but has a very good prognosis of success if the patient follows the postoperative behavior exactly (for example not abstaining from nicotine)..
The three-dimensional evaluation of the affected alveolar crest section by means of DVT is recommended before planning. So we can get an accurate picture of the bone deficit and the size of the required bone block. Also, this information can be meaningfully used to make a decision as to whether an individualized donor block should be better used after 3D data instead of a standard block size.
There are differences in the origin of the bone blocks:
1. Own bone blocks
These are taken from the patient in a place with good regeneration potential. Here you can find the ascending mandibular branch at the side of the wisdom tooth position. In our practice clinic, this bone is removed specifically with the piezosurgery procedure. Thus, the bone is protected and the losses caused by the preparation of the bone block are limited due to the thin working instruments. The removal of the bone from the iliac crest can nowadays be avoided as a rule. Only with very large defects (after accident, extreme atrophy or tumors) can such a procedure still be meaningful.
Advantages: high regeneration potential because granular, lower costs;
Disadvantage: additional surgical region for removal, thus higher trauma, postoperative swelling and higher OP risk, limited amount of knot;
2. Donor bone blocks
 A good alternative to self-bone grafting is represented by blocks of mesmeric donor bone (= human cancellous bone). A patented sterilization process ensures the highest level of safety during manufacture. The advantage is that human spongiosa in structure and composition corresponds to the own body tissue. After transplantation, the block is gradually streaked with newly formed bone and rebuilt into its own bone. We have a very good and extensive experience in the application of such bone blocks in our practice clinic. From our point of view, the prognosis for success does not differ from that of the self-inguinal blocks – with less trauma for the patients.
A good alternative to self-bone grafting is represented by blocks of mesmeric donor bone (= human cancellous bone). A patented sterilization process ensures the highest level of safety during manufacture. The advantage is that human spongiosa in structure and composition corresponds to the own body tissue. After transplantation, the block is gradually streaked with newly formed bone and rebuilt into its own bone. We have a very good and extensive experience in the application of such bone blocks in our practice clinic. From our point of view, the prognosis for success does not differ from that of the self-inguinal blocks – with less trauma for the patients.
Human spongiosa blocks are biocompatible and are well suited for maxillary and maxillary jaw construction.
Advantages: unlimited volume, no additional OP region, highly customizable, safe manufacturing process
Disadvantage: higher costs, additional education about donor bone
If there is a particular dilation or defect shape, using a 3D bone block may be the best way to regenerate your bone.
PDF-Download – Patient information on bone formation with human donor bones ***
3. Bone block after 3D construction (CAD bone block)
 As described above, the bone blocks are streaked by their own blood vessels and gradually replaced by patient bones. Prerequisite here is the absolutely precise fitting of the bone graft, whether its own bone or donor bone. With the 3D supported bone block technique, we can make you an absolutely defect-adapted bone block. The advantages are obvious: The precisely manufactured block no longer has to be adjusted by hand, this increases the throughput rate, significantly reduces the surgery time and even large defects can be treated very precisely with this technology. The planning is carried out according to the requirements for the subsequent supply of implants.
As described above, the bone blocks are streaked by their own blood vessels and gradually replaced by patient bones. Prerequisite here is the absolutely precise fitting of the bone graft, whether its own bone or donor bone. With the 3D supported bone block technique, we can make you an absolutely defect-adapted bone block. The advantages are obvious: The precisely manufactured block no longer has to be adjusted by hand, this increases the throughput rate, significantly reduces the surgery time and even large defects can be treated very precisely with this technology. The planning is carried out according to the requirements for the subsequent supply of implants.
How does the treatment work?
Once it is clear that there is a major defect, we produce a 3D image using low-radiation DVT. Afterwards we will discuss with you the defect situation and the subsequent planning. If there is a very extensive defect or a complex defect morphology, the recommendation for a 3D bone block may be. On the basis of the 3D data produced by us in advance, the bone block can then be virtually planned with the manufacturer and the size adjusted. It takes about 5 to 6 weeks until the block is manufactured individually for you using the same safe manufacturing process. On the day of the operation, the bone block is then conditioned and inserted and fixed at the planned location. With this technique, very large deficits in both width and height can be biologically compatible and supplied in the least traumatic way possible. A removal of larger blocks of autologous bone from the oral cavity or even from the iliac crest can be avoided with this technology.
Advantages:
Precise adaptation due to previous 3D milling, lower OP time, possibility to provide larger defects with one block;
Disadvantage:
significantly higher costs, additional education donor bone
Do you have any more questions about bone formation in Munich??
Related Posts
-

Bone structure of the jaw, jawbone construction. Hannover
Jawbone building in Hannover: So we give your dental implants firm hold What to do if the bone is missing? Then we build it up again! Implants need a…
-

Denture munich, creative dentists, dr
Denture in Munich Our shared secret. The lack of several or all teeth is a great challenge in everyday life for many people. Patient and dentist are…
-

General anesthesia Munich, creative dentists, dr
Dental treatment under general anesthesia in Munich Are you an anxiety patient or are you afraid of numerous painful procedures? Especially in large…
-

Dental insurance, dentist Munich, creative dentists
Which is the best dental supplement insurance for your dental treatment? It is well known: Good and high quality dentures is a costly affair. Quality,…